This data set has historical and projected information on the size of the susceptible population who are not immune to the coronavirus and at risk, the number of mild cases, the number of patients who are hospitalized, the number of patients who are in critical condition and need Intensive Care Units (ICUs), and the daily number of confirmed cases.
Based on the estimated needs for various types of medical resources, including ventilators, testing kits, and personal protective equipment (PPE), we calculate the corresponding demands in each state.
In terms of data on the supply of various types of resources, currently only the information on ventilators is available.
This model was originally developed by Alison Hill and adapted to our project. For a more detailed explanation, please visit:
https://alhill.shinyapps.io/COVID19seir/
The SEIR model reveals the transmission dynamics of a disease and resulting population flow amongst various groups based on disease exposure and evolution. The represented classes are as follows:
The susceptible class S, which contains those who are at risk and who have no immunity to the disease.
The exposed class E, which contains those who have contracted the disease but is asymptomatic and not yet infectious.
The infected class I, which represents those who have contracted the disease and are showing symptoms. It is further divided into three classes: I1 (mild cases at the onset of symptoms which do not require hospitalization nor ICU treatment), I2 (hospitalized cases), and I3 (those undergoing ICU treatment).
The recovered class R, which represents those who were previously infected and have recovered.
The deceased class D, which represents those who had been receiving ICU treatment who have become deceased.
Ventilator Demand
We assume that there is a constant percentage of ICU cases (I3) requiring ventilators. Estimated from historical data, the percentage we use here is 90%.
Testing Kits Demand
Given the rate that in the United States, around 1 out of 10 people is tested positive, we estimate the daily demand for testing kits to be 10 times the daily confirmed cases, or equivalently, 10 times the daily decrease in number of people in the susceptible group and the exposed group.
Personal Protective Equipment Demand
The number of personal protective equipment sets is estimated based on the needs of medical professionals for taking care of patients in different classes.
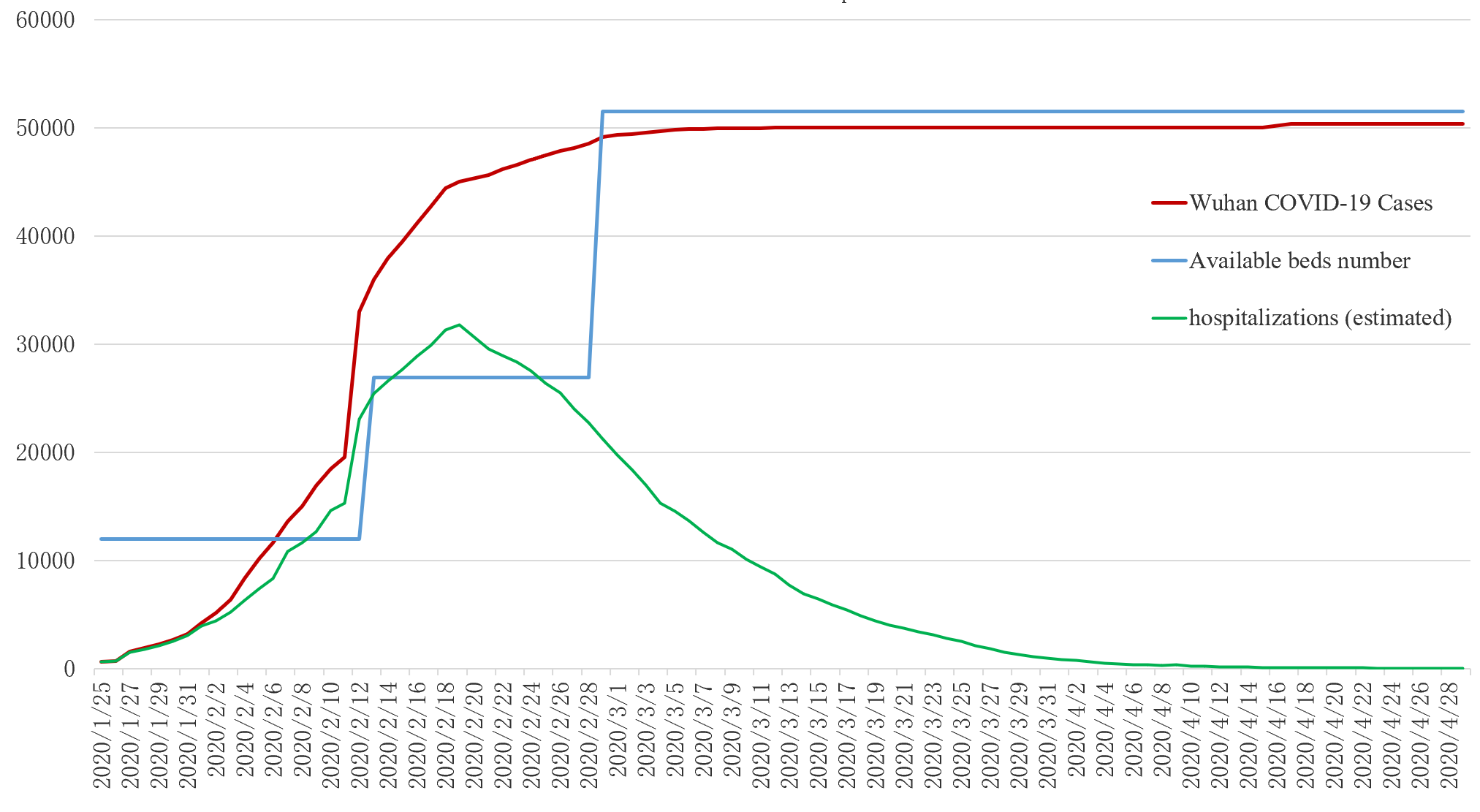
During the COVID-19 pandemic, hospitals in multiple locations reported shortages of hospital beds and ICU beds. For example, the following figure shows the demand and supply of hospital beds in Wuhan since the beginning of the outbreak. As the number of hospitalized patients surged, there was an apparent shortage of hospital beds in February. In order to address this issue, the local government increased the number of beds by requisitioning designated hospitals or building new makeshift hospitals.
Similar situations can be found in the US.
As projected by the Institute for Health Metrics and Evaluation (IHME)
, the demands of all beds or ICU beds in the second week of April are predicted to be 95% of the capacity, and over 20 states could be facing the shortage of beds in the worst scenario. In addition, this projection also suggests that the imbalance between supply and demand is regional, as the remaining states will have an oversupply of beds, and they could potentially be relocated and put to good use. Of course, the imbalance between demand and supply in each region is dynamic as the pandemic evolves, and therefore, in order to maximize the benefit from a coordinated resources allocation strategy and regional collaborations, the supply capacity in each region needs to be projected.
Factors that Affect Supply
Initial Stockpile
At the beginning of the pandemic, much of the demand needs to be fulfilled by the existing stockpile of resources, as it takes time for manufacturers and every participant in supply chains to adjust the production rate. The US federal government established the Strategic National Stockpile (SNS) in case of public health crises in 2002. The program was proved to be effective in the 2009 H1N1 pandemic. In the Contingency Planning section, we propose a method for calculating the optimal size of the initial stockpile, which minimizes both the shortage and the waste caused by oversupply. But in reality, the optimal level may not be attained for various reasons. The SNS has only been partially replenished since 2009, and thus getting quickly depleted in this COVID-19 pandemic. After the pandemic starts, it becomes more important for ex-post decision makers to estimate the existing stockpile and utilize it effectively.
Acquisition Rate
The rate of acquiring additional resources is determined by the production capacity and the capability to procure resources from elsewhere. For certain resources like PPE, studies have shown that although the US domestic manufacturing capacity is able to meet normal daily needs, it is challenging for the supply chain to immediately expand production in case of pandemics. Another source of supplies is the international market, which is associated with much uncertainty in pandemics, since shortages take place in a lot of places. For example, in April, the World Trade Organization (WTO) reported that
80 countries put restrictions on exports of personal protective equipment, such as face masks and gloves
.
Moreover, when facing a surge of demands and not being able to fulfill them all, suppliers often have to set priorities for orders, thus making it difficult to guarantee that different regions can all acquire adequate resources to fight against the disease. As an example, in the early stages of the outbreak of COVID-19 pandemic in the US, many state governments, local healthcare systems and the federal government were competing for resources in
a price-bidding war
, and oftentimes, state governments ended up paying higher prices for less resources. Therefore, at the regional level, the supply of resources can be difficult to predict if there is no coordination among regions, and thus addressing the regional imbalance between supply and demand is challenging.
Emergency Aquisition
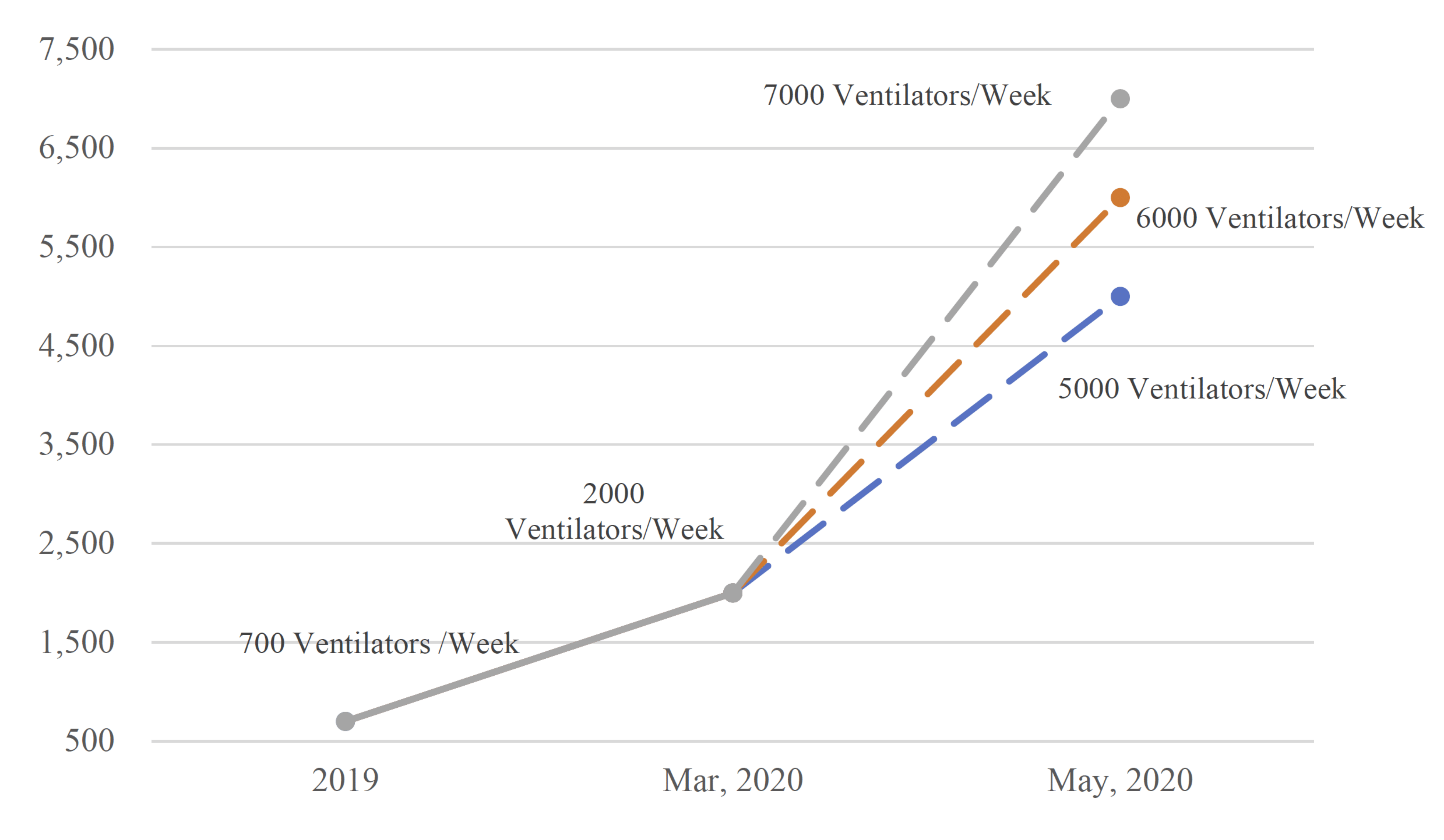
There is no easy way to change the initial stockpile once the pandemic starts, but remedies can be made through emergency acquisitions. The elasticity in production capacity can be possibly utilized to maximize the resources output. Around the time that SNS got depleted in April, President Trump invoked the Defense Production Act to mobilize manufacturers across the country to surge the production of medical resources like masks and ventilators. For ventilators, the following figure, created based on
data from the Advanced Medical Technology Association
, shows the drastic increase in production rate since March.
This website and its contents herein, including all data, mapping, and analysis ("Website"), copyright 2020 the University of Illinois, all rights reserved, is provided solely for non-profit public health, educational, and academic research purposes.
Use of the Website by commercial parties and/or in commerce is strictly prohibited.
Redistribution of the Website or the aggregated data set underlying the Website is strictly prohibited.
The Website relies upon publicly available data from multiple sources. The University of Illinois hereby disclaims any and all representations and warranties with respect to the Website, including accuracy, fitness for use, reliability, completeness, and non-infringement of third party rights.
Any use of the University of Illinois' names, logos, trademarks, and/or trade dress in a factually inaccurate manner or for marketing, promotional or commercial purposes is strictly prohibited.
These terms and conditions are subject to change. Your use of the Website constitutes your acceptance of these terms and conditions and any future modifications thereof.
Estimating Priority Vaccine Demand by State
Estimate Vaccine Demand for COVID-19 Priority Groups in 4 Simple Steps
The following figures demonstrate how centralized contingency planning can be done in the US with projected aggregate demands for ventilators, testing kits, and personal protective equipment.
You can adjust the costs in the "Planning Parameters" panel for various scenarios.
In our contingency planning model, we try to match the supply with the projected demand as close as possible, so that there is a minimum amount of shortage or surplus at each time point. In addition, the model takes production costs and storage costs into consideration for practicality. For example, if the marginal cost of producing and storing one unit of resource of a certain type (e.g., ventilator, testing kit, or personal protective equipment) outweighs the benefit it brings, then that unit is considered as excessive and should not be counted in contingency planning.
On this page, we use the projected aggregate demand in the United States to illustrate how contingency planning can be done.
Contingency Planning Based on Canada Aggregate Demand
The following figures demonstrate how centralized contingency planning can be done in Canada with projected aggregate demands for ventilators, testing kits, and personal protective equipment.
You can adjust the costs in the "Planning Parameters" panel for various scenarios.
In our contingency planning model, we try to match the supply with the projected demand as close as possible, so that there is a minimum amount of shortage or surplus at each time point. In addition, the model takes production costs and storage costs into consideration for practicality. For example, if the marginal cost of producing and storing one unit of resource of a certain type (e.g., ventilator, testing kit, or personal protective equipment) outweighs the benefit it brings, then that unit is considered as excessive and should not be counted in contingency planning.
On this page, we use the projected aggregate demand in Canada to illustrate how contingency planning can be done.
Choose States for Allocation
For demonstration purposes, this calculator allows you to select up to 5 states/provinces, so that the plots are legible. The model itself is not subject to the limit of number of regions.
After changing the selected states/provinces, please click the "UPDATE" button to see the updated results.
Resources Allocation Based on US State Demands
The following figures demonstrate how resources allocation can be done in the US with projected demands for ventilators, testing kits, and personal protective equipment in states that you select.
Ventilators
For therapeutic resources, we consider ventilators as representative examples, which is durable in the sense that they can be re-used once not being occupied. The demand of ventilator depends on severe ICU infected cases.
Testing Kits
For diagnostic resources, we consider testing kits as the prime example, which is also of single-use. We assume that systematic testing is conducted for people with mild symptoms.
Personal Protective Equipment
For preventative resources, we consider PPE as the representative example, which is single-use that they must be disposed after one time usage. The assessment of need for PPE sets varies by the patients and severity of medical conditions in care, and the function of medical professionals.
Model Description
In the time of severe resource shortage, a coordinated effort becomes necessary to deliver limited resources to where they are needed the most. New York City was among the first states to witness the COVID-19 pandemic. The state government issued an executive order to take ventilators and other protective gears from underutilized private hospitals and companies. As reported cases in NYC stabilized and decreased, the government shifted attention to other areas of potential outbreaks and allocated scarce resources accordingly. As one of the states with most aggressive pandemic responses, New York reported near zero COVID-related deaths since mid-July.
In this work, we consider the issue of optimal resource allocation in such a way that the overall economic cost of demand and supply imbalance is minimized. As regions may experience the pandemic in different stages, we can take a holistic approach to balance conflicting priorities and temporal differences of regions and the system. This work is an extension of the holistic allocation principle developed by
Chong et al. (2020)
in the context of insurance capital allocation.
Assume that the forecast of surge healthcare demand of various regions in a healthcare system can be obtained from predictive statistical models. The healthcare system with many regions is governed by a centralized authority, which makes financial and logistic decisions for all regions under its jurisdiction. The central authority can increase the total system wide supply by producing or importing additional supplies. While we consider the allocation problem at the start of the pandemic in this exercise, the demand projection should be closely monitored and regularly updated in practice to reflect the latest groundwork information.
The allocation problem arises when the system wide supply is unable to meet demands from all regions at all times. There are a number of circumstances under which the central authority may experience the need for allocation. First, the increase of total system supply may not keep up with the surge in demand over a short period of time. When the demand far exceeds the available system wide supply, the system can experience a
spatial competition
of resources. Second, it could be expensive to stock up regional inventories to meet short-term demand, due to transportation, disruption to supply chain, etc. One may have to take a cost-benefit analysis to assess its appropriate stockpiling size. Third, medical resources have different shelf life. Many sterile medical devices have short expiration dates. Disposable devices are typically intended for use on a single patient on a single procedure. For example, hospital beds, ICU beds, and ventilators can be regarded as durable medical resources; PPE and testing kits are considered perishable or single-use. Even if the system wide supply of single-use or perishable resources is sufficient at present, there could be a shortage down the road. Last, the central authority may anticipate a surge in demand at a later time and need to reserve a portion of newly acquired supplies for future use. In such a case, there could be a
temporal competition
of resources. In this work, we develop resource allocation methods that aim to strike the balance of spatial and/or temporal competitions, the cost and benefit of allocations, with respect to different shelf lives. Technical details of proposed models can be found in
Chen et al. (2020)
.
The exhibits above are derived from proposed allocation methods in this work and historical and projected demand data from
the Covid Act Now project
Choose States for Allocation
For demonstration purposes, this calculator allows you to select up to 5 states/provinces, so that the plots are legible. The model itself is not subject to the limit of number of regions.
After changing the selected states/provinces, please click the "UPDATE" button to see the updated results.
Resources Allocation Based on Canada Province Demands
The following figures demonstrate how resources allocation can be done in Canada with projected demands for ventilators, testing kits, and personal protective equipment in states that you select.
Ventilators
For therapeutic resources, we consider ventilators as representative examples, which is durable in the sense that they can be re-used once not being occupied. The demand of ventilator depends on severe ICU infected cases.
Testing Kits
For diagnostic resources, we consider testing kits as the prime example, which is also of single-use. We assume that systematic testing is conducted for people with mild symptoms.
Personal Protective Equipment
For preventative resources, we consider PPE as the representative example, which is single-use that they must be disposed after one time usage. The assessment of need for PPE sets varies by the patients and severity of medical conditions in care, and the function of medical professionals.
Model Description
In the time of severe resource shortage, a coordinated effort becomes necessary to deliver limited resources to where they are needed the most. New York City was among the first states to witness the COVID-19 pandemic. The state government issued an executive order to take ventilators and other protective gears from underutilized private hospitals and companies. As reported cases in NYC stabilized and decreased, the government shifted attention to other areas of potential outbreaks and allocated scarce resources accordingly. As one of the states with most aggressive pandemic responses, New York reported near zero COVID-related deaths since mid-July.
In this work, we consider the issue of optimal resource allocation in such a way that the overall economic cost of demand and supply imbalance is minimized. As regions may experience the pandemic in different stages, we can take a holistic approach to balance conflicting priorities and temporal differences of regions and the system. This work is an extension of the holistic allocation principle developed by
Chong et al. (2020)
in the context of insurance capital allocation.
Assume that the forecast of surge healthcare demand of various regions in a healthcare system can be obtained from predictive statistical models. The healthcare system with many regions is governed by a centralized authority, which makes financial and logistic decisions for all regions under its jurisdiction. The central authority can increase the total system wide supply by producing or importing additional supplies. While we consider the allocation problem at the start of the pandemic in this exercise, the demand projection should be closely monitored and regularly updated in practice to reflect the latest groundwork information.
The allocation problem arises when the system wide supply is unable to meet demands from all regions at all times. There are a number of circumstances under which the central authority may experience the need for allocation. First, the increase of total system supply may not keep up with the surge in demand over a short period of time. When the demand far exceeds the available system wide supply, the system can experience a
spatial competition
of resources. Second, it could be expensive to stock up regional inventories to meet short-term demand, due to transportation, disruption to supply chain, etc. One may have to take a cost-benefit analysis to assess its appropriate stockpiling size. Third, medical resources have different shelf life. Many sterile medical devices have short expiration dates. Disposable devices are typically intended for use on a single patient on a single procedure. For example, hospital beds, ICU beds, and ventilators can be regarded as durable medical resources; PPE and testing kits are considered perishable or single-use. Even if the system wide supply of single-use or perishable resources is sufficient at present, there could be a shortage down the road. Last, the central authority may anticipate a surge in demand at a later time and need to reserve a portion of newly acquired supplies for future use. In such a case, there could be a
temporal competition
of resources. In this work, we develop resource allocation methods that aim to strike the balance of spatial and/or temporal competitions, the cost and benefit of allocations, with respect to different shelf lives. Technical details of proposed models can be found in
Chen et al. (2020)
.
The exhibits above are derived from proposed allocation methods in this work and historical and projected demand data from
the Covid Act Now project
Pandemic
A pandemic is the worldwide spread of a new disease due to no or limited pre-existing immunity (ex. Covid-19). To mitigate pandemic risks, it is crucial for decision makers to understand the evolution of a pandemic and to assess potential impact resulting from the disruption of operation continuity.
Risk Management
In a time of great uncertainty, all organizations face the inconvenient truth is that pandemic risk is a certainty. Successful organizations utilize risk management techniques to reduce the financial impact of COVID-19.
Contingency Planning
Contingency planning helps organizations and governments prepare, respond to and control pandemics. While it is impossible to know the exact future, quantitative modeling based on best available predictive models can assist decision makers in assessing the severity of impact and developing stockpiling strategies for scarce resources.
Resource Allocation
Demand for critical resources often exceeds supply during a pandemic. Organizations are forced to make difficult decisions on rationing limited resources. This website offers quantitative tools to pool and allocate scarce resources, such as mechanical ventilators, testing kits and vaccines, among different geographic locations and over the course of a pandemic.
The research project aims to develop new quantitative framework and tools for public health decision makers and risk management professionals to assess COVID-19 pandemic risk and develop contingency and response plans.
The work represents a collaborative effort by researchers from the University of Illinois at Urbana-Champaign (United States) and Nankai University (China). This website is maintained and regularly updated by Illinois Risk Lab. Model details and instructions can be found in "Pandemic risk management: resources contingency planning and allocation" by Chen et al. (2020)
[Download]
.
Pandemic
Pandemic vs. Epidemic
Pandemic outbreaks are becoming more frequent
Pandemic brings risks to economics, business, health systems, and individuals
Risk Management
Identify risk
Analyze risk
Evaluate risk
Treat or rank the risk
Monitor and review the risk
Contingency Planning
Why contingency planning matters
Contingency planning for different indstries
Stockpiling Calculator
Resource Allocation
Spatial and temporal competition of resources
Improperly distributed PPE items can cause resource inefficiency
An
epidemic
is the rapid spread of disease to a large number of people within a given population. A
pandemic
is an epidemic that spreads to multiple countries or continents in a short amount of time. Usually, a pandemic is caused by the limited knowledge and immunity to a new pathogen. This is such the case for the 2019 novel coronavirus.
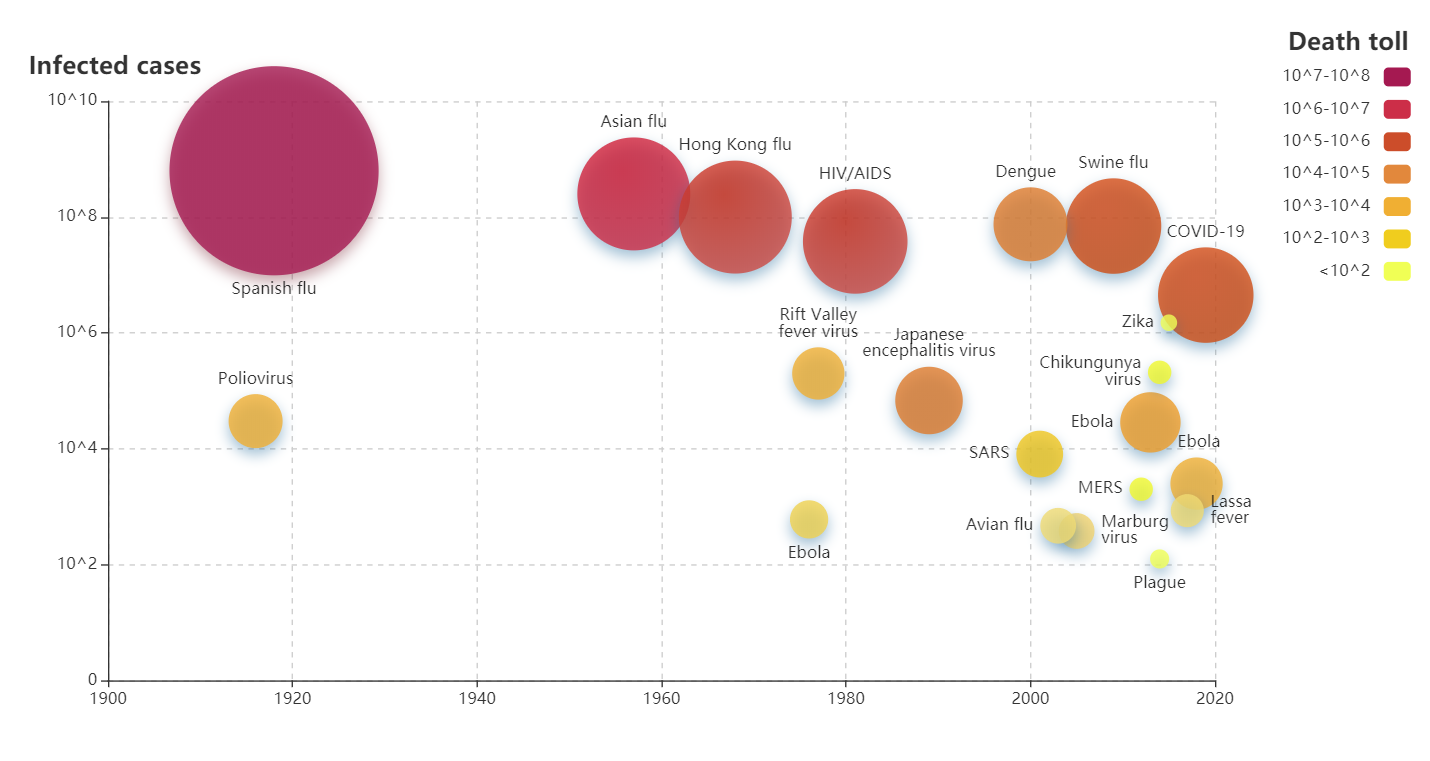
How Often do they Occur, and Just how Serious are They?
The following
graph
demonstrates both the frequency and severity of some notable epidemics since 1900.
The graph reveals that there have been thirteen impactful cases of infectious diseases that have occurred in just the first two decades of the 21st century. Some of them are even considered to be pandemic or pandemic-prone(e.g.
H1N1
,
Dengue
, and
Covid-19
. One
systematic study
shows that the diversity and the total number of outbreaks has had a significant global increase since 1980.
"This is a new normal, I do not expect the frequency of these events to reduce." warned Dr. Michael Ryan, the Executive Director of the Health Emergencies Program at World Health Organization in 2019 during an
interview with BBC
.
What Risks are Associated with a Pandemic?
This section demonstrates the challenges faced by the economy, businesses, healthcare systems, and individuals during this pandemic.
The Economy
A pandemic disrupts normal economic activities. Most governments implement public policies to slow down the spread of a pandemic. Their public policies can suppress productivity.
For instance, the policies involving the closure of businesses can negatively impact the economy by causing a drop in consumer spending to about
68% of the normal GDP
. In addition, the
estimated cost of SARS
related to the loss of economic activity is about $40 billion.
A risk facing the economy is the slowdown in its growth, which is indicated by a contraction in Gross Domestic Product (GDP). The U.S. Bureau of Economic Analysis (BEA) has estimated that there has so far been a
4.8%
drop in the U.S. GDP.
Additionally, a decrease in economic success results in the loss of tax revenue. The government often must cut down expenditures while fighting against the pandemic and will also reallocate resources to support nationwide healthcare systems.
Businesses
The risks faced by businesses include supply chain disruption, mandatory shutdown, and decreased labor force participation.
To control the spread of disease, many factories were required to close, which caused a demand-supply imbalance in the supply chain of various industries (such as the transportation industry). Such a disruption in the supply chain damages business material logistics and prevents the normal operation of affected companies.
Large unemployment rates also produce a huge financial burden on national unemployment insurance. For job-seekers, it becomes harder to survive in the job market due to the combination of the decreasing number of unoccupied jobs and the rise of those looking for work
Stores, restaurants, and all other business areas that were profiting from social interactions were also forced into lockdown due to government orders focused on reducing the spread of this disease. Some companies were able to adapt to this change by migrating their daily work to online platforms. Yet, businesses whose success was dependent on physical labor, such as grocery stores and
coffee shops
, suffered a great loss in their profit.
Because of the loss of profits and the increasing practice of implementing cost reducing plans during lockdown, many companies have been forced to
decrease their employee numbers or freeze their hiring processes
, which has caused massive pandemic-related unemployment. According to a
report by McKinsey
, it has been estimated that up to 53 million U.S. jobs are at risk for layoffs, furloughs and payment reduction. While certain expenses are saved due to the decrease in money spent on human resources, this decision for lockdown has decreased the labor force participation rate, making certain companies less productive. This problem can also be detrimental to the development of businesses after the pandemic.
A rapid increase in unemployment also leads to a tremendous burden on national unemployment insurance. Because of the decreasing number of job opportunites and the increase in job applicants, job-seekers are unable to find jobs. Thus, the government must allocate more of its budget towards providing unemployment insurance to protect those that have been affected.
Healthcare Systems
The main challenge faced by the healthcare system is the lack of medical resources during this pandemic. Medical resources are more likely to not be delivered on time due to the disruption of the supply chain and the lockdown of factories. With the growth of infected cases during the Covid-19 pandemic, most American hospitals have declared
shortages
of personal protective equipment (PPE). The PPE that are at its lowest stock includes medical masks, face shields, booties, gloves, gowns, hand sanitizer, disinfecting wipes, and thermometers.
Smaller healthcare institutions suffer more from the
broken supply chain
. During Covid-19, many American hospitals have relied on international supplied, especially those in Asia. Yet, most of the available supplies are required to be sold in large quantities or sell at an inflated price. Due to limited budgets, small healthcare institutions don't have the resource to outbid larger counterparts for medical materials.
Individuals
Pandemic risks facing common people can be divided into two categories: health related and non-health related
Health related risks include not only the presence of physical health and mental health problems caused by the pandemic, but also related medical costs. Infected individuals are burdened by many issues, such as paying for huge medical expenditures and lose a portion of their income due to hospital bills. Usually, physical health risks usually differ in different age groups of the population. For example, for Covid-19, older adults are at a
higher risk
for developing more serious symptoms.
The growing public fear of the Covid-19 pandemic generates many
mental health problems
, such as depression and suicide. The suicide rate is on the rise in
certain areas of the United States
due to development of mental health caused by social isolation and fear of the pandemic.
The non-health-related risks vary from person to person, but they are all related to financial loss. These include risks such as loss of income due to pandemic-related unemployment and excess expenses from inflated costs of necessary supplies.
The concept of
risk management
began as a means of analyzing and minimizing potential financial shortcomings. In general, the practice of risk management attempts to predict elements that have a potential to go awry and plan ahead to lessen levels of uncertainty. In recent years a risk analysis plan has become an important piece of success in countless sectors.
Examples of Risk Management Strategies in Practice
Still, the risk management process is highly variable to industry. For example, governments may use risk management strategies to handle issues related to domestic and international defense.
In the
insurance industry,
risk management is primarily used to assess and quantify the likelihood of events. An example of a potential current misstep in risk management strategizing can be seen through the extreme amount of unemployment uninsurance claims. Although the amount of claims are fairly unprecedented, a more successful plan would have accounted for the potential of surges to this degree.
Small businesses are beginning to
implement risk analysis plans;
an example of this is improving the security of a local business by installing security cameras around the premises to reduce potential crime.
Even on an individual level, risk management is an important tool. One way many people engage in risk management is by budgeting their expenses on a monthly basis, saving some money each month in case of an emergency.
Pandemic Risk Management and Strategies
We are currently living in a crucial time for risk management strategy development. The inevitable truth when dealing with a pandemic is that risk is a certainty.
Some of the most urgent risks
facing the United States in the midst of the COVID-19 pandemic aside from the obvious medical ramifications are:
A halted economy
Supply chain backup
Mass unemployment
Hiring freezes
Shortage of medical resources
Decreased labor force participation
Decrease in GDP
Growing public fear
These truly only scratch at the surface of the potential risks associated with a pandemic. Proper
contingency planning
paired with a coherent strategy for resource allocation can greatly manage the severity of some of these risks.
While pandemic risk management is a far reaching subject, we focus on the topic of resources planning and allocation in the work.
Contingency planning
in this context refers to risk management strategy developed prior to a pandemic that prepares for the potential imbalance of demand and supply in critical resources. Ideally, a contingency plan can help to control the risk that was accounted for and reduce the impact of its consequences. On the same note, resources allocation strategies are typically part of rapid response plans developed over the course of a pandemic that help to deliver resources to where they can be utilized in the most efficient way.
Our Mission Through a Risk Analysis Mindset
The CovidPlan team aims to provide insights for public health professionals to develop a comprehensive framework for pandemic risk management strategies. While pandemic risk management is not a new topic, there has been scarce literature on quantitative methods for combined strategies for stockpiling and allocations. It is our hope that this work can contribute to the growing body of scientific knowledge on the subject.
As the COVID-19 pandemic continues, we hope that the findings from this research work can provide some reference to public policy-makers on a quantitative basis for efficient allocation of limited resources. The allocation algorithms in this work are adaptive to the fast changing dynamics of the pandemic and demand-supply imbalance. The framework of contingency planning presented in this work may also be used by decision makers for developing strategic stockpiling plans for the next pandemic.
A
contingency plan
is a plan devised for an outcome other than in the usual (expected) plan. Contingency plan ensures the continuity of business operation and protects enterprises from the shortage of resources, minimizes disruption to the supply chain and identifies key staff, assigning specific responsibilities for rapid responses and recovery.
The main purpose of pandemic contingency planning to address potential uncertainties as a result of unexpected pandemic outbreak such as COVID-19. Many industries and organizations responded quickly in the early stage of the pandemic owing to their well-thought and adequate contingency plans.
Why is Contingency Planning Important?
Repeated history of epidemics has shown that pandemic risk is inevitable. Contingency plans help us prepare for the eventuality of pandemics. Many businesses nowadays still do not have a developed contingency plan for a pandemic. Based on a study by JP Morgan Chase Institute, companies with fewer than 500 employees have less than a month of cash reserves on average. Moreover, the likelihood for a pandemic to result in a high rate of absenteeism, disruption to supply chains, disruption to business travel could create a devastating impact on companies. Therefore, it is crucial for companies and markets to have a contingency plan to prepare for pandemics.
How Do We Plan for Contingency?
Contingency planning is recommended by the Center for Disease Control and Protection (CDC) for organizations in all sectors.
Businesses
Businesses create contingency planning by assessing the impact of a potential pandemic on their operations, and develop concrete plans for employers and customers. The CDC created a
checklist
for businesses in preparation for a pandemic outbreak based on the following steps:
Plan for the impact of a pandemic on the business
Plan for the impact of a pandemic on employees and customers
Establish policies to be implemented during a pandemic
Allocate resources to protect employees and customers during a pandemic
Communicate to and educate employees
Coordinate with external organizations to help the community
Education
Universities and other educational institutions set up contingency planning with the priority on personnel safety, preventative measures such as virtual delivery of education. CDC also created a
checklist
for educational institutions to prepare for pandemic flu. The checklist for educational institutions include following:
Promote the daily practices for everyday preventive actions at all time
Provide flu-preventions supplies in the school
Plan for staff and students' absences and keep track of the flu-related absences
Plan ways to increase space or limit face to face interactions between people
Develop a risk-management process for the school
NIST seven-step process
The National Institute of Standards and Technology (NIST) defines contingency planning as management procedure or policies designed to maintain or restore business operations. The NIST defined a
seven step contingency planning process
for developing and maintaining a viable planning program.
Identify any specific regulatory requirements related to contingency planning
Conduct a business impact analysis (BIA) to identify and prioritize critical system, business processes, and components
Identify and implement preventative controls and measures to reduce the effects of disruptions, increase availability, and reduce contingency costs
Define recovery plans to ensure critical systems can be restore quickly
Develop contingency plans containing detailed guidance and procedures to recover from disruptions
Plan testing, training, exercises to reinforce, validate, test contingency plan
Maintain contingency plan as living documents. Update them regularly to reflect changes to influential factors
How Does the Government Prepare for a Pandemic?
Adequate preparation and plan prior to pandemic requires the establishment of infrastructure and capacity, which could take for many years to fully develop. Thus, the government plays a significant role in overall coordination and coummincation to help create contingency planning.
The United States government has developed three tools to guide national, state and local planning and response. These tools align with the
World Health Organization's (WHO) global framework
of pandemic phases and risk assessment activities for preparedness, response, and recovery.
This framework is used to guide influenza pandemic planning and provides recommendations for risk assessment, decision-making, and action in the United States. It describes the progression of an influenza pandemic using six intervals.
This is an evaluation tool developed by CDC and external influenza experts that assesses the potential pandemic risk created by influenza.It assesses potential risks of pandemic based on two different scenarios -- "emergence" and "public health impact".
This framework is used when a novel influenza A virus is identified and it is spreading from person-to-person in a sustained manner. It determines the impact of the pandemic based on clinical severity -- how severe is the illness due to the infection -- and transmissibility -- how easily the pandemic virus spreads from person-to-person.
Pandemic Influenza Plan
In 2005, the
United States Department of Health and Human Services
(HHS) developed a
Pandemic Influenza Plan
to coordinate and improve efforts to prevent, control, and respond to A(H5N1) viruses as well as other novel influenza A viruses of animal (e.g. from birds or pigs) with pandemic potential. The plan provides a high-level overview of the approach that government will take to prepare for and respond to a pandemic, which contains
three pillars
:
Preparedness and communication
The U.S will work to improve the international community’s capacity and the commitment to take coordinated, effective action to contain an outbreak at its site of origin if possible and if not, to slow or limit its spread.
Surveillance and detection
The U.S will develop, enhance, and encourage early implementation of international screening and monitoring mechanisms to limit the spread of viruses with pandemic potential. Additionally, the government will work to ensure effective surveillance, rapid detection, and transparent reporting of outbreaks internationally by strengthening scientific and epidemiological expertise abroad.
Response and containment
The U.S will work to ensure nations and relevant international organizations agree as soon as possible on a doctrine of international response and containment to implement in the event of a human outbreak.
Contingency Planning Development
While a full fledged contingency plan requires more sophisticated planning, this research work focuses primarily on the stockpiling of medical resources. In particular, we consider healthcare contingency plans for stockpiling to contain three steps:
Identify key resources needed
Critical medical resources can typically be categorized into therapeutic resources, preventative resources, and diagnostic resources. Different organizations may require varying quantities of these resources.
Forecast demand
To avoid the shortage of supply to meet a surge in demand, we need to predict and assess the magnitude of demand for various types of critical resources. Such demand forecasts require the modeling of multiple factors driving the demand.
Develop a stockpiling strategy
The next essential planning strategy is to develop a stockpile or repository of these medical resources, which can provide a buffer to increase supply at the time of an actual pandemic.
How Does the Government Respond to a Pandemic?
When a pandemic occurs, the Federal Government responds to the situation as quickly as possible to provide guidelines, make sure enough medical funding, and implement policies such as travel restrictions, social distance, etc. Local health authorities also need to cooperate with each other to provide leadership and guidance on the actions that are necessary.
Federal funds rates were lowered by 150bp in March to 0-0.25bp. Purchase of Treasury and agency securities in the amount as needed.
The Federal Reserve also introduced facilities to support the flow of credit.
Federal banking supervisors encouraged depository institutions to use their capital and liquidity buffers to lend, to work constructively with borrowers affected by COVID-19.
Lower the community bank leverage ratio to 8 percent. Provide extension transition for the Current Expected Credit Loss accounting standard.
What is a Centralized Stockpiling Strategy?
A
centralized stockpiling strategy
is intended to provide a stopgap measure to meet the surge in resources demand at the early stage of the pandemic. A practical stockpiling strategy is often based on an act of balance between adequate supply and economic cost. During a pandemic outbreak, the central authority needs to secure additional resources based on forecast of future demand and to allocate existing resources across various subsidiaries in accordance to their local conditions.
Strategic National Stockpile
An example of Centralized Stockpiling Strategy is the
Strategic National Stockpile (SNS)
, which is a repository of antibiotics, life-support medications, IV administration, airway maintenance supplies, and medical/surgical items. It is designated to support healthcare systems with any public health threat. The role of SNS is to supplement medical or protection supplies during public health emergencies. It serves as a buffer when there is a shortage of medical equipment like ventilators during pandemics like COVID-19.There is $7-8 billion worth of emergency supplies stored in 12 different secret warehouses located strategically around the country.
If a healthcare facility needs supplemental ventilators or other medical supplies from the SNS during a public health emergency, it should work through the state public health department. State health officials are the ones who can request federal assistance for supplies, including ventilators.
Existing Problems with Current National Stockpile Strategy
Medical countermeasures (MCMs)
are medical supplies that supervised by the U.S. Food and Drug Administration (FDA) that can be used to diagnose, prevent, protect from, or treat conditions associated with chemical, biological, radiological, or nuclear (CBRN) threats, emerging infectious diseases, or a natural disaster.
Several existing problems with the SNS have been discussed at the
Nation's Medical Countermeasure Stockpile Workshop
, where the nation's top experts addressed opportunities to improve the efficiency, effectiveness and sufficiency of current national stockpile. Among many other matters, the following are most relevant to the purpose of this research work.
The SNS lacks sufficient resources
to maintain existing inventory. Since March 2020, U.S hospitals have already reported shortages of critical equipment needed to care for seriously ill patients. However, at the same time, SNS only has about 10 percent of its total inventory stockpiled, since the inventory was not replenished quick enough prior to the COVID-19 pandemic and the lack of resources supply.
The SNS should not only deliver Medical Countermeasures (MCMs) to local public health authorities, but also
support local-level dispensation efforts
, provide clinical guidance about the use of MCMs, and implement the appropriate systems to monitor treatment compliance during adverse events.
The current SNS model is not sustainable:
the SNS cannot continue to buy MCMs for an ever-expanding list of material threats; it needs to integrate across these threats in conjunction with the
Public Health Emergency Medical Countermeasures Enterprise (PHEMCE)
, which is designated to coordinate Federal efforts to enhance Chemical, and Biological threats,as well as disease preparedness, and make critical decisions about what to buy and what not to buy given its resource constraints.
The purpose of this research work is to provide new quantitative models to develop stockpiling and allocation strategies. While it is unrealistic to assume that these new models would address all of the above-mentioned issues, we hope this work could contribute to the public knowledge on the subject and inspire decision makers to utilize more quantitative tools in their efforts to combat pandemics.
When there is a severe shortage of critical resources, like the one experienced during COVID-19, a coordinated effort to obtain supplies and manage existing resources becomes essential. Not all states experience an equal surge in demand at the same time. Therefore it can be argued that the federal government should track the current use of resources and project the need of resources in all states to coordinate the allocation of resources. In doing this, the state can avoid both shortage and surplus. Resources that need to be distributed during a pandemic include perishable and durable resources. Examples of perishable resources include PPE, testing kits, and IV fluids. Examples of durable resources include hospital beds, ICU beds, and ventilators. There are many reasons that resources would need to be actively monitored and allocated in the midst of a pandemic.
Why resource allocation?
Supply and Demand
The increase of total system supply may not keep up with the surge in demand over a short period of time. When the demand far exceeds the available system wide supply, the system can experience a spatial competition of resources.
Expense
It is expensive to stock up regional inventories to meet the demand over a short period of time, due to transportation, disruption to supply chains, etc. One may have to take a cost-benefit analysis to assess its stockpiling strategy.
Different Shelf Life
Medical resources have different shelf life. Many sterile medical devices have short expiration dates. Disposable devices are typically intended for use on a single patient on a single procedure. On the other hand, durable medical resources such as hospital beds and ventilators last a while.
Anticipated Demand
Central authority may anticipate a surge in demand at a later time and need to reserve a portion of newly acquired supplies/raw material for future distribution or production. One aspect of resources allocation is to manage temporal competition of resources.
Macro vs. Micro Pooling
There are two sects of
resource allocation
: macro level resources pooling and micro level rationing. Macro level resource pooling describes resource allocation at the macroeconomic level. In macro level resource pooling, a central authority acts in the best interest of a union of many regions to increase supply as well as coordinate the distribution of existing and additional resources among different regional healthcare providers. Micro level rationing describes resource allocation at the microeconomic level. In micro level rationing, individual hospitals have to make difficult but necessary decisions to ration limited existing resources as well as new supplies.
While in both cases the aim of allocation is to deliver limited resources to where they are most needed, the macro level pooling addresses more of the spatio-temporal differences and the micro level rationing addresses more of the healthcare effectiveness and justice. The setting of standards, protocols, and policies can have a profound impact on the functioning of a healthcare system at the time of a crisis. Therefore, the best practice of resource allocation should be based on scientific assessment and evaluation rather than in the moment decisions. To put it more simply, resource allocation must follow a set of rules.
Allocation Rules
Holistic Approach
A
holistic approach
aims to take into account many different facets of hospitals and patients in order to decide where the resources are best put to use. It seeks to strike a balance among different objectives for various stakeholders.
Optimization Objectives
The
optimization approach
aims to follow a set of conditions that optimize the way that resources are distributed. There are many different ways optimization conditions can be formed.
Minimization of Shortage and Oversupply
One optimization condition seeks to minimize shortage and oversupply. Authorities must allocate more resources to epicenters of a pandemic than other regions under less immediate threat.
Promoting and Rewarding instrumental Value
This optimization condition details that critical preventive gears and medical care be provided first to healthcare workers in the front line and employees in essential businesses and critical infrastructures. The society bears heavy economic cost when these workers fall ill and are unable to return to work.
Prioritizing the Worst Off
This optimization condition details that access to critical medical treatment should be reserved for patients facing life-threatening conditions, when there is an insufficient supply of equipment such as ventilators.
Maximization of Benefit from Treatment
This optimization condition details that individuals with the best chance of survival should be given treatment before individuals with the least chance of survival. Following this logic, access to ventilator treatment should be prioritized to patients with the highest chance of survival, patients who are younger and can benefit the most from treatment.
Examples of Resource Inefficiency
GetusPPE.org Statistics
The statistics from
GetusPPE.org
showed a lot of resource shortages. For example, 22% of institutions surveyed reported that they had no N95 respirators remaining. Additionally, 36% of institutions surveyed had no face shields remaining. A quote from an institution surveyed by GetusPPE.org emphasizes the severity of the situation saying, "We are out of everything. Providers using one mask for 3+ weeks. Many COVID patients. Zero gowns. Great need. Large academic hospital."
Peru Oxygen Shortage
There is a
shortage of oxygen
in Peru, where coronavirus is hitting hard. Oxygen is one of the main tools keeping patients alive. As a response to the shortage of oxygen, black markets have emerged which has led to immense price gouging. Before the price gouging, one cylinder of oxygen cost $353, but now on the black market it costs as much as $1,470. Many people are dying because they are unable to find or afford oxygen. A quote from someone in Peru in desperate need of oxygen exemplifies the severity of the situation in Peru saying, "I feel helpless, angry, and furious, I feel like my hands are tied. My father is sick and we cannot afford something that is so essential for him to survive." In addition to the oxygen shortage, Peru faces an extreme lack of hospital beds having less than two hospital beds per 1000 people.
This model reveals the evolution of the optimal allocation of supplies between two regions based on their demands. The resources demanded are durable, which means that they have a prolonged shelf life, and the available supplies are to be completely distributed amongst the two regions. A ventilator is an example of an important durable resource used for treating patients with coronavirus.
This model reveals the evolution of the optimal allocation of supplies between two regions based on their demands. The resources demanded are perishable, which means that they have a limited shelf life, and the available supplies are to be partially distributed amongst the two regions. This means that there will be supplies left over after distribution to the regions. Personal protective equipment (PPE) are examples of important durable resources used for treating patients with coronavirus.
The research project aims to develop new quantitative framework and tools for public health decision makers and risk management professionals to assess COVID-19 pandemic risk and develop contingency and response plans.
The work represents a collaborative effort by researchers from the University of Illinois at Urbana-Champaign (United States) and Nankai University (China). This website is maintained and regularly updated by Illinois Risk Lab. Model details and instructions can be found in "Pandemic risk management: resources contingency planning and allocation" by Chen et al. (2020)
[Download]
.
Contact Us
We are open to professional partnership and sponsorship for this project,
which provides invaluable experiential learning opportunity
for student associates of Illinois Risk Lab. If you are interested in collaboration,
please contact us using the form below.












{kind=link}